



Ineligible for Healthcare
Our healthcare system is imploding.


“I believe that you go right for the jugular." said Michael Fox.
07/11/2025: 8:22 am - DAPHNE, AL, USA
It is as true today as it was 50 years ago when Martin Luther King, Jr., so rightly said:
“…of all forms of inequality, injustice in health is the most shocking and inhumane.”
Unfortunately, these injustices in access to care are a demonstrable result of our current broken and failed healthcare system. And now Congress makes worse the U.S. healthcare system in order to feed the wealthy.
Unsustainable and irresponsible political promises and corporate and individual greed have created this flawed U.S. healthcare system—one that is too expensive and costs twice that per capita compared to the rest of the Western world.

I give up. Why are we getting worse healthcare results? Any ideas? There should not be a for-profit scam while poor people go without any healthcare whosoever. What kind of people are we?
Currently the US, compared to similar Western countries, has the lowest life expectancy at birth, highest reported maternal and infant mortality, highest hospitalization rate from preventable causes, highest death rate for avoidable and treatable conditions, highest suicide rate, and highest chronic disease burden rate in the world. That only costs us twice as much.
In a U.S. nutshell, people are too poor to get healthcare coverage. Healthcare tied to your employment means the unemployed can die right after eating their cake.
In essence, we are spending more than any other civilized country in the world and getting markedly worse results. No other known industry in a competitive or many noncompetitive societies could survive by being twice as expensive while producing markedly inferior products, services, and results.
The U.S. healthcare system is so badly flawed that most experts believe it will now likely implode, creating devastating effects on our country's health and economy. Hospitals will close, and those jobs will be irreplaceable.
As a nation, we cannot and should not continue to support or tolerate a system that threatens the quality, safety, accessibility, and affordability of its citizens’ healthcare.

The claim denied scam has been widely exposed. Some insurance companies begin with claim denied.
We are going to have to reform toward health equity, also known as "health justice”. Simply ensure everyone has the opportunity to reach their highest level of health, regardless of their identity, income, or location. That is equitable, but it is not what we are doing. Why is having good health insurance pegged to having a job that provides for health insurance? There is something inherently inequitable right there.
Health justice requires equal access to resources, power, and opportunities to make health decisions. Health justice focuses on correcting practices that create health inequities and inequality. Those are the health disparities we must wipe out.
Health disparities are preventable differences that populations experience in the burden of disease, injury, violence, or opportunities. When people have limited access to health-fulfilling and health-sustaining resources, they are more likely to experience health issues. Health inequities are differences in health status or in the distribution of health resources between different population groups, arising from the social conditions in which people are born, grow, live, work, and age.
Health inequities are unfair and could be reduced by the right mix of government policies. We are going backwards because healthcare is such a large part of our monthly outlay.
The new CR bill is unquestionably the biggest step backward for both healthcare and a fair tax system in modern American history. We must correct this with the 2026 midterms and 2028 elections.
The conditions in which people are born, grow, work, live, and age are social determinants of health (SDOH). Long-standing inequities in the 6 areas influence health outcomes and quality of life. Understanding these inequities can help us improve health outcomes and promote health equity.
Social and Community Context. Social context includes the human interactions where one lives, works, learns, plays, and worships. Special programs help protect the health and well-being of people who experience disadvantage. Social and community context also includes discrimination (the unfair treatment of people or groups based on their race, gender, age, or sexual orientation). Discrimination—including racism—can be found in many societal systems beyond healthcare, including housing, education, criminal justice, and finance.
Healthcare Access and Use. Some groups that have been marginalized face multiple barriers to accessing health care. Structural barriers include socioeconomic status, lack of insurance, transportation, childcare, or ability to take time off work to visit a doctor. Barriers to patient-provider interactions and healthcare quality also include cultural differences and language barriers.
Neighborhood and Physical Environment. Access to public transportation, supermarkets, and healthcare contribute to segregation of American cities. Discriminatory practices limit housing options to neighborhoods with inadequate funding for school districts, higher crime rates, poorly resourced infrastructure, and limited access to nutritious, affordable foods. These conditions can make illnesses, diseases, and injuries more common and severe among discriminated groups.
Workplace Conditions. Occupational health inequities are avoidable differences in work settings. Physical and mental health outcomes are linked to social, economic, and environmental disadvantages. Other workforce factors include temporary work arrangements, socio-demographic characteristics (e.g., age, sex, race), and organizational factors (e.g., lack of safety measures, limited or no health insurance).
Education. Inequities in access to high-quality education commonly affect people who have been historically marginalized. Lower-quality education leads to lower literacy and numeracy levels, lower high school completion rates, and barriers to college entrance. Educational barriers limit future job options and lead to lower paying or less stable jobs.
Income and Wealth Gaps. Other barriers to good jobs include geographic location, language differences, discrimination, and access to transportation. Financial challenges make it difficult to manage expenses and access affordable quality housing, education, nutritious food, and reliable childcare.
The U.S. healthcare system struggles with a lack of health equity. Clearly, lower-income individuals and minority groups experience poorer health outcomes and face discrimination. Key issues that are causal:
High Costs. The US spends more on healthcare than any other developed nation, yet life expectancy is lower, and chronic disease rates are higher. High costs, especially for prescription drugs and insurance deductibles, lead to cost-related delays in care.
Inadequate Access. Many Americans struggle to afford healthcare, delaying or skipping needed care due to costs. This includes those with employer-sponsored insurance, marketplace plans, Medicaid, and Medicare.
Uneven Quality. There are significant disparities in healthcare quality and outcomes across different demographics and geographic locations. Lower-income individuals and minority groups often experience poorer health outcomes and discrimination.
Cybersecurity Vulnerabilities. A cyberattack on Change Healthcare, a major healthcare clearinghouse, disrupted claims processing and payments, highlighting the vulnerability of the healthcare system to cyber threats.
Ethical Issues. Ethical concerns include patient privacy, transmission of diseases, end-of-life issues, and relationships between patients and providers.
Corporatization. The U.S. healthcare system has been corporatized. It is now controlled by a decreasing number of increasingly powerful conglomerates where profit is often the main metric of performance and success. The stark realities of this dark devolution create daily difficulties for patients trapped in this harsh and inequitable system.
A frequent, disturbing type of patient encounter highlights the essence of this decay. Often when suggesting the need for a particular surgery to a patient they will rarely ask the most obvious and important questions such as: “Will I have significant pain? Is it dangerous? Can I die?”
Instead, they more commonly ask: “How can I pay for this? Will I lose my house or my job? How fast can I get back to work?,” followed, all too frequently, by comments like: “There is no way I can afford this. I don’t have access to that level of deductible. This will bankrupt me.” And, periodically, they would come to this decision: “I just can’t proceed, doctor. This will put my family in the street. I’ll just tough it out and take my chances.”
There is something deeply and fundamentally wrong with this increasingly common situation where the accessibility of healthcare, which I believe should be a basic human right, is determined by one’s financial station in life. For this to be occurring in the most affluent country in the world is not just wrong, but abjectly amoral.
The U.S. healthcare system leaves too many people out. That results in 26 million uninsured and 43 million underinsured. In fact, recent World Health Organization metrics suggest that the US does an incredibly poor job with healthcare delivery, with the US ranked 37th overall to comparable Western country metrics and last among the 11 highest-income countries. These rankings are not surprising when you consider the fact that the US healthcare delivery system consumes 17% of our current gross domestic product and is the leading cause of personal bankruptcy accounting for 66.5% of total U.S. individual monetary defaults.
Placing Profits over Patient Care. The U.S. healthcare system handicaps business competitiveness with a crippling 160% increase in employer healthcare costs in the last 20 years, which averages about $14,000 per employee. This system also causes downward pressure on employee wages resulting in a 8.9% inflation adjusted decrease in employee household income. In addition, it requires many Americans and their families to line up in fields for humanitarian healthcare events mirroring the activities of many third-world countries as well as requiring increasing numbers of citizens to use the ER as their default medical care.
This default is fragmented, costly, inefficient, and a generally poor method of providing care with a total lack of continuity. This healthcare model also drives significant racial disparities in the availability and quality of care, and in the outcomes for these patient populations.
Over the past several decades, many inadequate policies, negative influencers, and societal and demographic changes have come together to impact our already failing healthcare system.
Ten states have not expanded Medicaid under the Affordable Care Act (ACA). These states are:
Alabama,
Florida,
Georgia,
Mississippi,
South Carolina,
Tennessee,
Texas,
Kansas,
Wisconsin, and
Wyoming.
The first 7 are previously slave states and still deeply racist. Alabama, my home state, is racist and one of the states that has not expanded Medicaid. Alabama would see significant changes to its healthcare landscape if it were to expand the program under the Affordable Care Act (ACA). Potential impact on Alabamians:
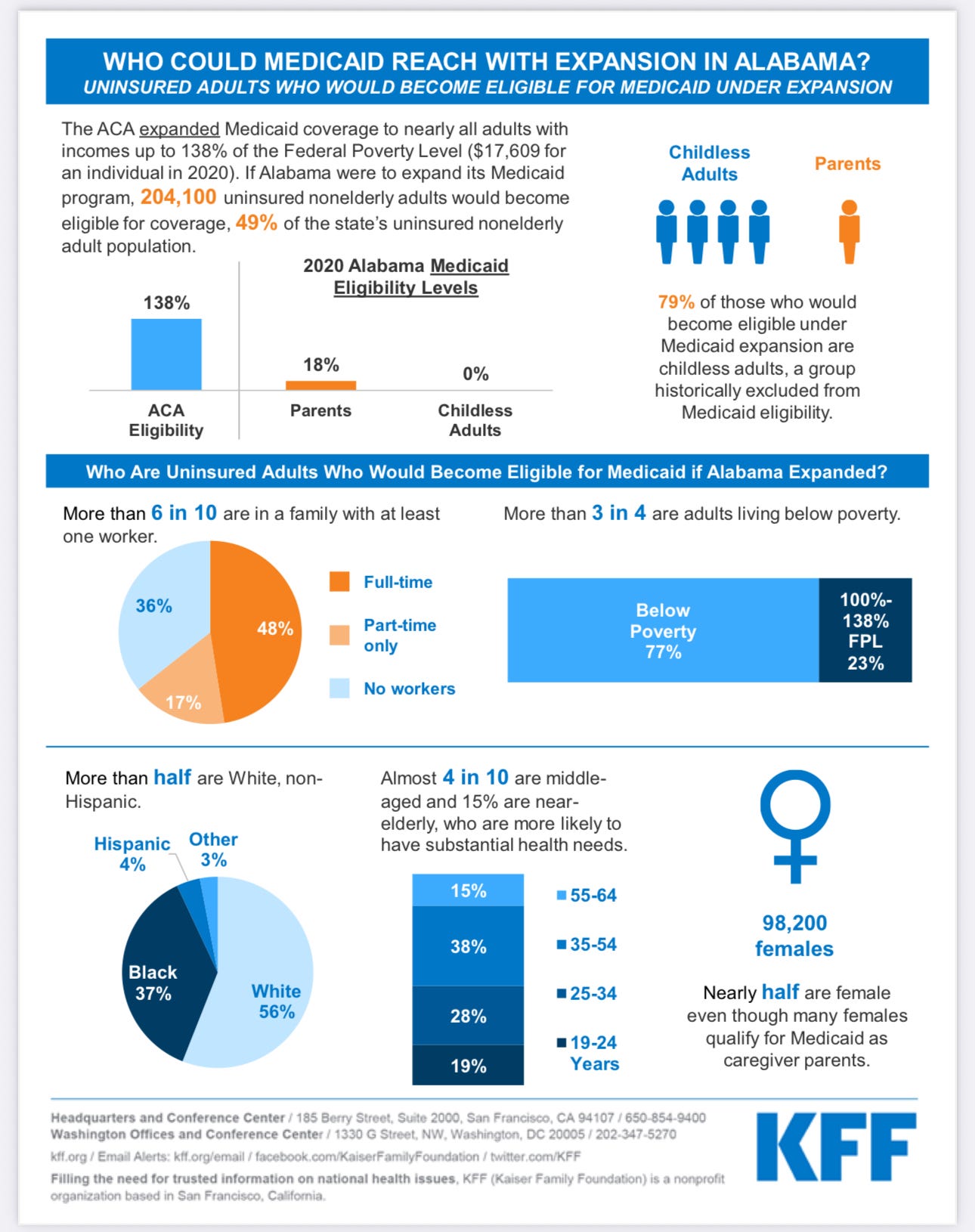
Expanded Coverage. Currently, Alabama Medicaid has very limited eligibility for adults, particularly parents and no coverage for childless adults. Expansion would extend eligibility to nearly all adults with incomes up to 138% of the Federal Poverty Level (FPL) which was $17,609 for an individual in 2020.
Reduced Uninsured Rates. Over half (56%) of the uninsured adults in Alabama who would become eligible for Medicaid if it were expanded are White, non-Hispanic individuals, according to a Kaiser Family Foundation (KFF) analysis. (The organization was formerly known as the Kaiser Family Foundation but since became KFF.) Thus, a significant portion of white Alabamians who currently lack health insurance could gain coverage.
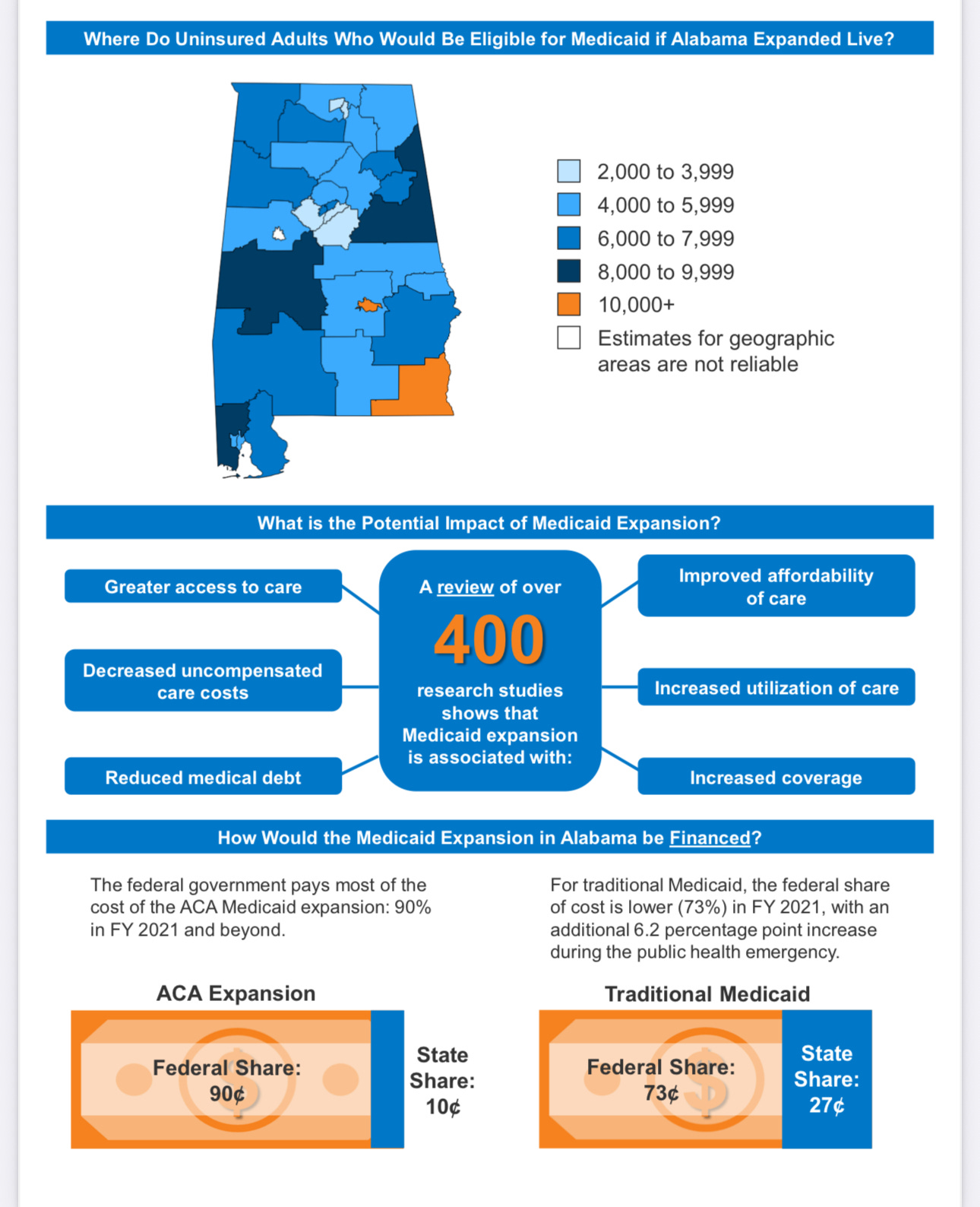
Improved Health Outcomes. Studies show a link between Medicaid expansion and improved health outcomes, including earlier cancer diagnoses, better management of chronic conditions, and lower mortality rates, according to KFF. This could lead to a healthier population in Alabama.
Economic Benefits. Medicaid expansion has been linked to economic benefits for states, including increased economic growth. This could lead to job creation and improved financial security for all Alabamians.
Current eligibility and the coverage gap:
Alabama's current Medicaid eligibility for parents and caretaker relatives is very low – up to 18% of the FPL.
Many low-income working adults, including those working minimum wage jobs, fall into a "coverage gap" where their income is too high to qualify for Alabama Medicaid but too low to receive subsidies for private insurance on the Marketplace. This affects a substantial number of working Alabamians, including white individuals.
Arguments for expansion:
Humanitarian. Expansion could reduce suffering and provide peace of mind to families struggling with healthcare costs.
Economic. Medicaid expansion could bring billions of federal dollars into the state's economy, generating tax revenue and creating jobs. This would also include bolstering the workforce as individuals would have better access to healthcare and thus be better able to work.
Strengthening the Healthcare System. Expansion could help financially struggling hospitals, particularly in rural areas.
HOT BUTTONS is a reader-facing periodical from a business development executive (retired) driving to provoke thought. To receive new perspectives, become a free or paid subscriber.
We can forge our better fate in 2026 only if we can build a foundation inspiring enough of our voters to weigh in. Let us demand a coherent platform.
In the meantime, we must take to the streets en masse on July 17 to honor Rep. John Lewis, a civil rights icon. We can surpass the June 14th protesters in numbers. That was 11 million to 13.4 million. I hear both.
This month, let us go out there 20 to 25 million strong!!! And yell, as Jackson Brown sang, til you go down. Yes, take to the streets.
With your subscriptions I can write this newsletter. I’m grateful to everyone who sponsors me, and one thing I want to add:
Thank you for finding my voice. You have given that a place and a meaning.
Please share. Please become a paid subscriber if you can as it keeps me writing. Thank you for reading.
Right on Carl. Being the recipient of not one but two transplanted lungs, hip replacement and dental reconstruction due to side effects of steroid-based medication, I know all too well that what you present here is in fact true based on my personal experience.